A Non-Obvious Inflection in Diet Drugs: GLP-1’s Expanding Regulatory and Therapeutic Footprint Beyond Obesity
GLP-1 (glucagon-like peptide-1) drugs have disrupted obesity treatment paradigms, yet a subtle but consequential shift is unfolding: positioning GLP-1 therapies as multi-indication platforms influencing regulatory frameworks, capital flows, and industrial structures across diabetes, renal disease, dementia prevention, and even food systems. This inflection remains under-recognized despite its potential to reshape healthcare industrial strategy and regulation over the next 10–20 years.
Obesity treatment via GLP-1 agonists like semaglutide has attracted broad attention, but emerging developments—including expanded Medicare coverage, new FDA indications, and experimental dementia trials—signal a widening of GLP-1’s clinical and regulatory footprint. This paper examines how these signals may coalesce into structural shifts that transcend conventional obesity therapeutics, with implications for payers, manufacturers, regulators, and health systems.
Signal Identification
This development qualifies as an emerging inflection indicator. While GLP-1 drugs are known primarily as anti-obesity agents, recent additive approvals and trials reveal a pivot to multi-system therapeutic applications (obesity, type 2 diabetes, chronic kidney disease, dementia prevention), which collectively could transform their role from niche weight-loss drugs to foundational medicines for metabolic and neurodegenerative disorders.
The time horizon for this structural change is medium to long term, estimated at 10–20 years, with a high plausibility band given current regulatory momentum and investment. The sectors exposed include pharmaceutical manufacturing, health insurance and reimbursement, regulatory policy, food and beverage innovation, and chronic disease management.
What Is Changing
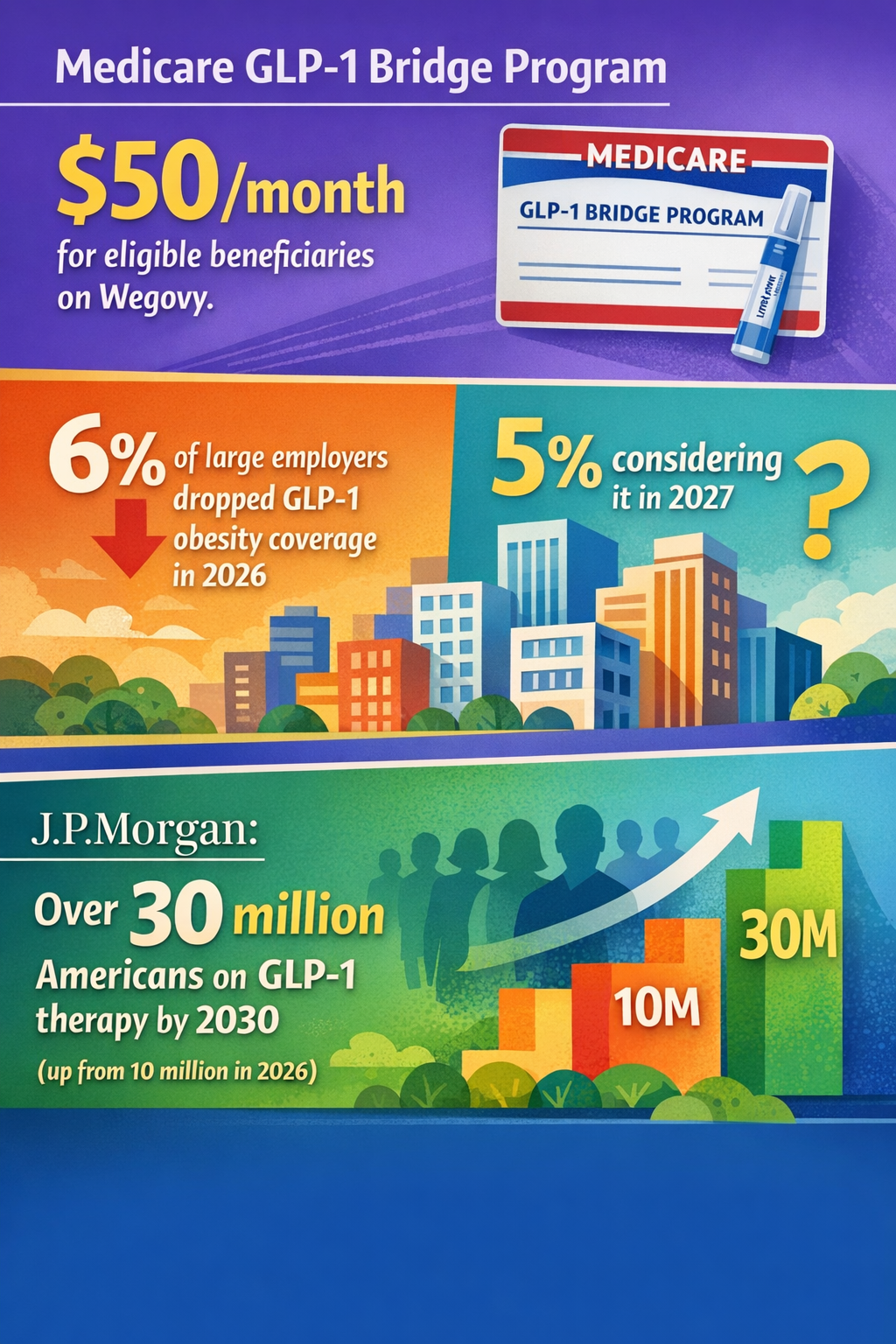
Obesity-focused GLP-1 treatments such as Wegovy and Ozempic have gained significant traction, with Medicare’s new GLP-1 Bridge Program offering discounted access to eligible beneficiaries starting in 2026 (Noom 15/03/2026). This represents a shift in reimbursement policy signaling official recognition of GLP-1’s clinical value beyond lifestyle interventions. Moreover, if Congress expands permanent Medicare coverage for these therapies after 2027, payer dynamics could fundamentally change (Medical Daily 22/04/2026).
Meanwhile, the U.S. Food and Drug Administration (FDA) has approved indications of semaglutide (marketed as Ozempic) for reducing kidney disease progression and cardiovascular death in patients with type 2 diabetes and chronic kidney disease—underscoring GLP-1’s transition into multi-morbidity pharmacotherapy (Goal BMI Wellness 06/02/2026). Complementing this, a major $100 million trial launched to assess whether GLP-1 agonists combined with lifestyle changes can reduce dementia risk (PharmaPhorum 01/05/2026). This is a structurally distinct therapeutic direction, extending GLP-1’s scope beyond metabolic syndromes into neurodegeneration.
On a parallel front, GLP-1 driven changes in eating patterns are forecasted to influence food and beverage innovation, with companies anticipating shifts in product development toward flavors and functional foods that complement altered appetite regulation (Food Ingredients First 28/03/2026). This suggests a systemic, cross-sector extension of GLP-1 effects into consumer behavior and supply chains.
Counterintuitively, some large employers have reduced GLP-1 obesity coverage, possibly due to cost control imperatives (Resourceful Finance Pro 10/01/2026). This points to complex payer dynamics and potential bottlenecks in mass adoption, particularly in fragmented private insurance.
Disruption Pathway
At the core is a causal shift from monolithic indication drug development toward pharmaceutical platform strategies, where the same molecular class addresses multiple comorbidities. The conditions accelerating this include increasing prevalence of metabolic and neurodegenerative diseases as aging and obesity trends persist, combined with significant public and private R&D investments.
Regulatory adaptations—such as Medicare’s GLP-1 Bridge Program—lower patient cost barriers and set precedents for reimbursement in adjacent indications, encouraging manufacturers to invest in broader clinical trials and label expansions. This in turn stresses existing insurance models, which must reconfigure coverage policies across multiple disease states and potentially rationalize formularies.
The evolving pharmaceutical-industrial complex may respond by vertically integrating R&D pipelines to produce comprehensive metabolic-neuro therapeutics portfolios, shifting capital allocation away from tightly focused drug development toward multi-indication platforms. Feedback loops emerge as positive clinical outcomes (e.g., kidney disease risk reduction and dementia delay) bolster payers’ cost-benefit calculations, incentivizing wider coverage and patient uptake, which further enhances manufacturer revenues and R&D budgets.
Unintended consequences may include increased regulatory complexity as agencies grapple with multi-indication approvals and off-label use controls, alongside potential liability exposures if long-term side effects (e.g., fluid balance risks highlighted in heat illness advisories) manifest in vulnerable populations (ABC News 18/02/2026).
If dominant regulatory and payer models adapt by embracing outcomes-based reimbursement tied to multi-disease endpoints, this could permanently shift the governance architecture away from single-condition silos to integrated care value frameworks, with strategic positioning favouring manufacturers and providers capable of delivering cross-indication treatment regimens.
Why This Matters
The decision relevance lies in anticipating a multi-layered transformation in how GLP-1 therapeutics are positioned, valued, and regulated. Capital allocation may pivot as pharmaceutical firms prioritize platform development and longitudinal patient engagement models over short-term obesity drug launches.
Regulatory frameworks could evolve to accommodate complex label expansions and real-world evidence requirements, challenging traditional safety and efficacy assessment paradigms. For payers and insurers, risk pooling and benefit design will need recalibration to manage cross-disease therapy costs and long-term savings, possibly triggering new reimbursement models.
Competitive positioning in the pharmaceutical sector may consolidate around organizations capable of integrated clinical development and data collection across metabolic and cognitive health. Supply chains in the consumer food sector might adjust to align with changing appetite and nutritional demand profiles induced by GLP-1 use, a less visible but significant downstream industrial impact.
Governance implications include managing new safety risks (e.g., hydration challenges) and liability shifts as drugs extend beyond obesity into fragile patient groups. The confluence of extended indications and expanded market access programs could redefine stakeholder relationships among manufacturers, regulators, payers, clinicians, and consumers.
Implications
This emerging inflection could plausibly scale into structural change in drug development paradigms and reimbursement policies. GLP-1 products may become foundational medicines that cross traditional specialty boundaries, impacting capital flows and health system design.
It is unlikely that the current view of GLP-1 drugs solely as weight-loss agents will persist unchanged; instead, multi-indication strategies may become the norm.
However, this is not inevitable. Adoption depends on trial outcomes, cost-effectiveness analyses, payer willingness, and regulatory agility. Alternative interpretations may emphasize payer resistance or adverse event risks as limiting factors, potentially resulting in restricted market expansion or segmented use cases.
Early Indicators to Monitor
- Legislative or regulatory changes expanding permanent Medicare coverage beyond 2027
- FDA approvals or breakthrough therapy designations for non-obesity GLP-1 indications
- Venture funding or M&A activity targeting companies developing GLP-1 platform therapies for neurodegenerative or renal indications
- Emergence of value-based reimbursement contracts incorporating multiple GLP-1 related endpoints
- Food and beverage product launches explicitly designed for GLP-1 altered appetite profiles
Disconfirming Signals
- Decisive negative trial results halting dementia or kidney disease indications
- Legislative rollback or failure to extend Medicare GLP-1 bridge coverage
- Broad-scale payer cuts or exclusions of GLP-1 coverage due to cost or adverse events
- Regulatory tightening in approval processes limiting label expansions
Strategic Questions
- How should pharmaceutical R&D and commercial strategies adjust to capture multi-indication GLP-1 opportunities?
- What regulatory adaptations and payer models will best incentivize safe and equitable multi-disease GLP-1 deployment?
Keywords
GLP-1; Medicare coverage; Multi-indication therapeutics; Drug regulation; Dementia; Obesity treatment; Healthcare reimbursement; Pharmaceutical industry; Food innovation; Chronic kidney disease
Bibliography
- If Congress acts to expand permanent Medicare coverage of GLP-1 drugs for obesity, the coverage picture after 2027 could change. Medical Daily. Published 22/04/2026.
- The new Medicare GLP-1 Bridge program will allow eligible Medicare beneficiaries to get certain weight-loss GLP-1 medications, including the Wegovy injection and pill, for $50 a month. Noom. Published 15/03/2026.
- FDA approves Ozempic for a new indication: reducing the risk of worsening kidney disease and cardiovascular death in adults with type 2 diabetes and chronic kidney disease. Goal BMI Wellness. Published 06/02/2026.
- A large-scale trial has been launched, with $100 million in backing, to explore whether lifestyle changes coupled with GLP-1 agonists or similar incretin therapies can reduce the risk of dementia. PharmaPhorum. Published 01/05/2026.
- 6% of large employers dropped GLP-1 obesity coverage in 2026, and another 5% are planning to or are actively considering it in 2027. Resourceful Finance Pro. Published 10/01/2026.
- Foodology has identified GLP-1 - driven eating patterns as one of seven trends expected to shape F & B development in 2026. Food Ingredients First. Published 28/03/2026.
- The Centers for Disease Control and Prevention recommends drinking two to four glasses of fluids each hour for prevention of heat-related illness, a goal that might be harder to achieve for patients on a GLP-1. ABC News. Published 18/02/2026.